Face Recurve
THE FACE RECURVE® CONCEPT
What is the Face Recurve® ?
Face Recurve® , a concept recently developed and published by the Le Louarn /Buthiau/Buis team, offers a new understanding of the mechanisms at play in structural ageing of the face. This new concept has allowed elaborating adapted treatments thanks particularly to new medical and surgical techniques which, in turn, provide for introducing a new global strategy (preventive and curative) in the struggle against structural ageing.
What is the Face Recurve® ?
Structural ageing of the face
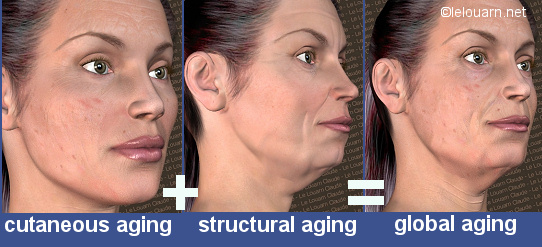
First of all, it is important to differentiate between cutaneous ageing and structural ageing. Actually, these two components of global ageing of the face cannot be explained by the same logical mechanism and do not respond to the same treatments:
Cutaneous aging involves change that takes place over the course of time at the outer coating level, i.e., the skin. It is manifested by a loss of elasticity (the creased and thinned out appearance), discoloring (dyschromia or pigment spots), red blotches, dilated pores… The use of botulinum toxin in cosmetic therapy over the past 15 years has evidenced the role of the expression muscles in cutaneous ageing of the face. By reducing maximal muscle contraction, which means reducing slightly the degree of expressiveness also, it is possible to prevent the occurrence of certain wrinkles and fine lines (such as, for instance, crow’s feet or an incipient leonine line but not the naso-labial fold). Other sun-caused fine wrinkles and lines are better treated through an abrasive technique (laser, peeling, dermabrasion).
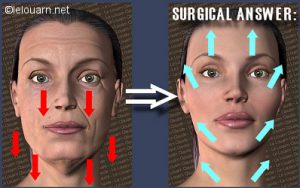
Structural aging involves the deep layers: bone-fat-muscle. It is manifested by a hollowing of the paramedian furrows (placed symmetrically on each side of the face): tear trough (hollowed rings under the eyes), naso-labial folds, bitterness folds, cervical bands and occurrence of excess volume areas (bags under the eyes, jowls…) and subsequent sagging of the facial tissues. To date, the treatments that were proposed consisted in the filling of the furrows and folds (using fillers or fat) and/or in pulling back the skin via the facelift. Both propositions had an inconvenient: that of a possible puffy look caused by the filling procedure, when maximum effect was sought (too much filler), or of a possible pulled appearance (skin pulled too tautly with the facelift).
The difficulty lay in the fact that gravity was unanimously implicated as the foremost cause of structural ageing. With one accord, scientific publications put the responsibility on gravity for facial ptosis, whilst a few fixed points were thought to hamper uniform tissue descent. This gravity/fixed points combination had to lead to the creation of furrows and to the overlying collection of fat. From this standpoint, surgical treatment was aimed at pulling upwards, i.e., “lifting”.
However, several signs seemed to point to the fact that this theory (gravity + fixed points => structural aging) might not be a valid one.
Firstly, the results obtained via conventional facelift surgery often yield esthetic improvement at the cost of a certain transformations of the face.
Since it could not provide the true structural appearance of a young persons’ look, surgery often would end up (especially in cases of repeat treatments) with smooth faces which had, nevertheless, a « pulled » look and, hence, unfortunately hardly unnoticeable features like: cheekbone skin lifted too high towards the temples, cheek-level hollows causing a shadow extending from the mouth to the ear with a persisting naso-labial fold; smoothed out neck though still marked by the cervical bands… If indeed structural ageing was due to gravity, the lifting of the tissues should not transform the face but restore its young appearance.
Secondly, certain aspects of structural aging seemed quite difficult to cure with conventional surgery.
In some cases, surgical treatment of certain structural aging-associated stigmata would require very taut pulling (even risky at times) and would, therefore, lead to incomplete or inadequate correction (as in the case of the naso-labial fold, for instance) or involve a risk of subsequent scar enlargement or even of necrosis in cases of very excessive pulling. Where other locations were concerned, however, the outcome of surgery could prove unstable over time (eg. the bitterness fold and the jowls) or insufficient (eg. the cervical bands when they have been little touched upon while the remainder of the face has been smoothed out). As regards conventional palpebral surgery, the problem also arises of a certain resulting bony-looking, rigid gaze, associated with a persisting hollowing aspect of the rings under the eyes in spite of the fact that the excess skin has been remedied.
Furthermore, analysis of structural aging from photographs obtained of female patients who could provide pictures of themselves when they were young and older do not fit with the theory of « gravity » and «fixed points ».
As a matter of fact, when comparing these photographs, the following could be observed:
1 – On the upper face
In some cases, the eyebrows have descended in the course of time, while in other cases they have gotten higher on the forehead although one would logically expect that they should always descend under the effect of gravity, the final appearance due to gravity-related ageing being that of lowered eyebrows in all cases.
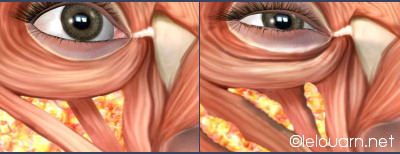
A hollowing is to be noted in the inner upper corner of the eye (beneath the eyebrows): this upper-lid furrow is the upper continuation of the tear trough. Such hollowing can give the gaze a somewhat “bony” appearance. The inner aspect of the inner upper lid is evidently hollowed upwardly, whereas, according to the gravity theory there should logically be a cutaneous bulge apparent inwardly, as seen outwardly.
Instead of there being horizontal lines (indicating tissue sagging), the upper circum-orbital wrinkles run vertically (right across the eyebrows to cause frowning).
As time goes by, the lower lid seems drawn upwards. It covers more of the bottom part of the iris, which causes the eyes to look smaller with age, while the lower eyelid should logically drop and widen the gaze downwards.


2- On the mouth
In most cases, with age, the lower lip is thinned out and, more particularly, it curves in inside the mouth in its mid portion. Gravity-related aging, however, should cause the lower lip to be everted and dropping centrally.
3 – On the cheeks
The lines on the cheeks run vertically and the excess skin is found between the lines. As described by anatomists, gravity combined with fixed points should lead, in fact, to the creation of horizontal jugal folds, with sagging originating from those fixed points.


and fixed point theory doesn’t correspond to reality of ageing
4 – On the jowls
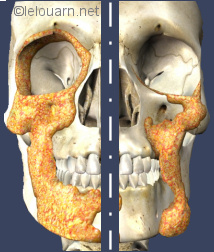
With time, there is often a concavity that forms between the chin and the jowl, together with a loss of volume at this point. The appearance resulting from gravity-related aging should, however, yield the same volume both in front of and behind the fixed point with arch-shaped sagging lines reflected to that fixed point. There is no reason for such volume loss to run through the entire height of the bitterness line.

the jowl (in yellow), should gravity theory apply the aspect would be quite different (in orange)
5 – On the neck
The right and left cervical bands become prominent with time, and are separated by a hollow. A gravity-caused appearance should yield slack cervical skin centrally at the most, but not on the sides, for there is no known fixed point at this median neck level.

cervical bands is not compatible with the gravity theory
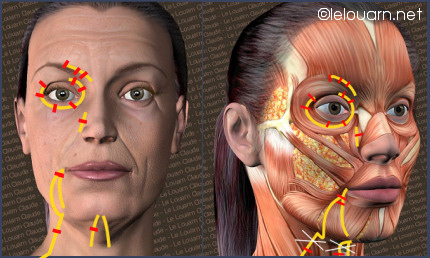
Lastly, analysis of the facial expressions of young subjects shows that very young people can actually mimic the structural aging at the various region levels by contracting their facial muscles.
For example, when pouting, one causes the same bitterness and jowl lines to appear as in those occurring in an elderly person at rest. When expressing despise or disgust, the raised nostrils cause the naso-labial fold to be more marked, as seen in ageing. By contracting the front of the neck, young subjects cause vertical cervical bands to appear similarly to those which are visible in elderly people at rest. But how could one mimic the effect of gravity on one’s face? If young persons can mimic the effects of structural aging by using their muscles, it then seems probable that the latter are involved in this type of ageing.


How was Face Recurve® invented?
Dr Le Louarn had studied the aging effects on gaze for a considerable period of time, and more particularly those relating to the hollowing of the rings around the eyes. It was difficult for him to imagine how gravity could be responsible for the more marked appearance of the rings with age, since such half-circular hollowing of the rings takes place deeper to the bone as time goes by, whereas the tissues should logically be descending vertically (towards the mouth), especially considering that, anatomically, there is not fixed point in that region of the face.
As an officer once said to a young sergeant who was trying pointlessly to understand why a certain hill that was clearly indicated on the general staff map was missing from the field: « If reality does not match the map, it must mean that the map is wrong » . In the case of structural aging, it seemed particularly appropriate to reconsider the commonly accepted theory.
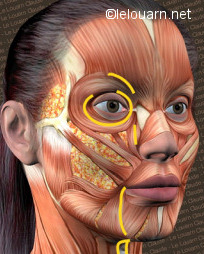
In dynamic anatomy, Dr Le Louarn’s works on the aging of the gaze had lead him to observe that the contraction of a specific segment of the malar portion of the orbicularis oculi muscle and, more particularly, its upper part, could be responsible for the hollowing of the rings under the eyes. He had noticed that each time this muscular segment contracted, as in the forced blinking reflex, it took bearing on the edge of the orbital bone. It could be possible that the thousand-time repeated contraction of this segment would cause, in time, the fat tissue between this muscle and the bone to be expelled upwards, thereby creating the bags, and downwards where the malar bag is created, thus causing a hollowing of the ring at rest (as hammer and anvil).

More generally, considering the face as a whole, surgeons and anatomists have long been able to observe a structural difference between the face of a young person and that of an elderly subject. In young subjects, deep-lying facial fat is found in large, located conglomerates deep to the muscles, while superficial fat which is located between the skin and the muscle forms a uniform coat under the skin.
In the elder subject, however, deep fat tissue is decreased and superficial fat is increased, the latter being disposed more irregularly. It is then conceivable that the million-time-over repeated muscular contractions during facial expression would cause the fat to be expelled and progressively lead to a more marked hollowing and to the formation of deeper furrows at rest, with referred excess volumes developing.
Morever, the use of botulinum toxin in cosmetic treatments has lead Dr Le Louarn to think that the muscles implicated in facial expression might shorten in the course of time (as opposed to a widely recognized idea to the effect that they should actually get longer and more relaxed in the same way as the skin under the influence of gravity). In concrete terms, for example, if one could smooth out a crow’s feet wrinkle and loosen and relax the muscle by injecting some botulinum toxin into it, this would mean that ageing causes that muscle to retract.

Hence, in order for muscular contraction to cause the fat lying deep to the furrows to decrease and superficial fat to increase and create volume masses, a young muscle would have to be convex-shaped and long at rest and be rectilinear and shorter upon contracting. With age, the muscle would have to shorten and to lose its convexity (i.e., remain in the contracted state). This could be the only logical explanation for the transfer of fat tissue during contraction.
If this theory was to be valid, it had to be verifiable:
– A radiological study had to evidence a shortening of the muscle with loss of convexity thereof with age (or on contraction).
– Additionally, the theory had to prove compatible during anatomical dissection.
– Last but not least, it had to be clinically applicable in the treatment of structural ageing and, therefore, to provide for the introduction of new technical avenues toward improving treatment efficacy.
Radiologist Didier Buthiau (Institut de Radiologie de Paris) has conducted MRI studies of sequences and constants which might bring forth evidence of muscular curvature. This was the great moment of truth designed to show that this theory was correct. Dr Buthiau then carried out a series of films on his own and then asked the surgeon to tell, from the pictures, whether the subject was young or old based on the curvature of the muscles and the distribution of the deep and superficial fat tissue layers. The test proved conclusive! In young subjects at rest, the muscle is convex with fat lying deep to the structure. In time, the same becomes straighter and shorter while the deep-lying fat becomes thinner and superficial fat increases.
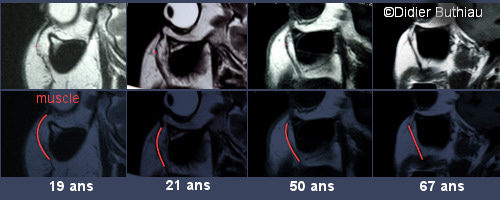
The great mechanism involved in structural aging could henceforth be studied more closely. The model of a rectilinearly-tending and fat-expelling muscle is the theoretical foundation upon which rests the Face Recurve® concept.
The Face Recurve® concept
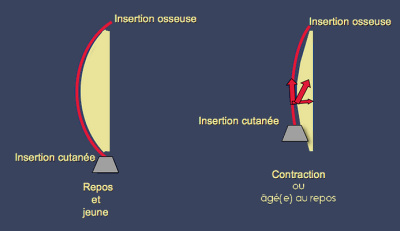
The facial expression muscles run typically from the bone deep to the skin. In young subjects, they are curved at rest. This convexity is achieved thanks to the underlying deep fat tissue layer. They become rectilinear and expel the fat transiently upon contracting. On loosening, the muscle becomes completely relaxed again while the fat tissue resumes its original position.
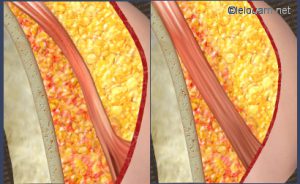
When contracting itself, the expression muscle retracts and shortens
in doing so, it looses its convexity and pushes the deep fat toward the surface
The role of this convexity in young subjects is twofold. First, the cutaneous insertion of the muscle is more forward, extruding. Secondly, the muscle is curvilinear, longer and its contraction range is wider. The facial expression is therefore more projected, wider and more revealing when the subject is young. In order to look younger, one must therefore try to preserve one’s range of expressiveness and not become set in one’s facial expressions, although reduced contraction is needed to treat the mimic lines (as a matter of fact, when we tell a person that they look tense – which is the opposite of the relaxed condition, we are not paying them a compliment).
In the elderly subject, age and repeat contractions cause that the muscle no longer can relax totally (in medicine, one refers to increased resting tone); it is shorter, more rectilinear and, hence, the difference between its contracted and relaxed states (the range) decreases and this is noticeable. Consequently, the elderly person’s face is more marked and tense.
Should muscle tissue as a whole be implicated uniformly in the transfer of fat, with age the face would present wide hollows corresponding to the respective surfaces of the mimic muscles, whereas it is rather marked by specific hollows with referred volume masses. As an example, at the lower eyelid level there is no hollowing extending from the lashes to the middle of the cheekbones due to the Orbicularis Oculi which forms a large ring around the eye, but merely a clearcut crease : the tear trough itself, while the bags under the eyes and the malar mould increase volume-wise.


Actually, certain fascicles are more particularly involved than others in the transfer of the fat tissue, thereby causing structural aging. An anatomical study has shown that these are usually located most deep to the furrow for which they are responsible. Furthermore, their functional role has been shown to be quite limited: therefore these fascicles have been called Age Marker Fascicles (or AMF).

AMFs are primarily responsible for paramedian structural aging of the face. They are directly implicated in the appearance of the bags under the eyes, the hollows related to the tear trough, the naso-labial and bitterness folds, the jowls and the cervical bands. With age, they alter the face structurally so as to indicate the latter’s biological status (doubtless intended for the preservation of the species).
Anatomically, the Age Marker Fascicles present an identical shortening phenomenon, although the same is highly enhanced as compared to the remainder of the muscle, which has two consequences:
– As the AMFs become shorter and more rectilinear, the underlying fat is expelled from beneath the concavity of these fascicles to be transferred laterally. The fatty volumes thus transferred cause the bags under the eyes to increase in volume, the malar mould (areas beneath the eye rings) and the volume above the naso-labial folds, the jowls and the double chin.
– Since the age marker fascicles are inserted within the skin folds, a shortening thereof, comparatively to their initial lengths, create excess skin and volume. The paramedian folds are made apparent: glabellar fold, tear trough, naso-labial fold, bitterness fold and cervical bands.
Unfortunately, both these phenomena (fat transfer and muscle fascicle shortening) are the more efficient facial age markers as the contours thus induced (fat-generated volume increase and hollowing of the folds), enhance mutually their visibility. Regarding the oval of the face, for example, a shortened muscle induces the hollow marking the bitterness fold, while the deep-lying fat volume that is transferred towards the surface and rearwards causes the jowls to appear. Thus, one element reinforces the other…
Gravity does not come into play until much later to affect the cutaneous and fat tissues, which have already been damaged through AMF muscular action, thereby causing sagging. The apple does not fall off the tree because of gravity, but because it is ripe; gravity is merely responsible for its falling vertically.
Good news! Clinical and anatomical studies of the age marker fascicles have shown the latter not to be indispensable to the patient, as their functional role is either weak or nil. It is therefore possible to hamper their deleterious action or to correct the consequences thereof without causing any harm, while preserving the natural looking expression of the face.
Plastic surgeons Le Louarn and Buis have conducted a substantial work of literature analysis and dissection to determine the sites most adapted to carry out impairment procedures and/or resection in these little studied areas. Naturally, clinical experience has provided for developing specific surgical and medical techniques. Thus, Face Recurve® has not only caused a real turnabout of the way the mechanism of structural aging of the face used to be thought of, but it has lead to profound changes in the anti-age therapeutic strategy for structural aging both surgery- and medicine-wise.
Face Recurve® : surgical and medical techniques adapted to the mechanisms of structural aging.
Inasmuch as Face Recurve® has made it possible for a new understanding of the aging process to take place, a set of medical / surgical techniques aimed at countering specifically the deleterious action of the age marker muscle fascicles could be developed. The intent of these techniques is to preserve or restore the anatomic structure, so as to have it match as closely as possible that of a young individual.
This they can do by:
– hampering the action of the AMFs (weakening of such by injecting botulinum toxin or through precise surgical resection),
– masking (using fillers) or correcting fat tissue transfers (through surgical restitution thereof to its right place).
The following explanations regarding the procedures aim to permit a good understanding of the Face Recurve® concept. Practical information regarding the hereinafter medical and surgical procedures (indications, therapeutic alternatives, involved risks, recovery…) are to be seek in the files to which they refer : “Fillers: rejuvenation injections”, “Botulinum toxin”, “Eyelid/ Blepharoplasty surgery” and “Facelift Face Recurve® lift”
Medical techniques
Botulinum toxin injections
As a preventive measure, botulinum toxin can be used to forestall AMF shortening. The same is then injected only to decrease the muscle resting tone without curtailing its maximum contraction strength. Such an injection has little bearing on facial look (results are little apparent at rest and not at all on contraction); therefore, it is actually only recommended in cases when a person’s physical appearance plays a major professional role and when prevention is a sufficient motivation.
Further into the ageing process, Botulinum toxin is still used to act on muscle resting tone but, more typically, in other places it is also used to curtail contraction and, hence, to act on facial expression lines like crow’s feet. The treatment is evident both at rest and on contraction.
Following Face Recurve® -type surgery, botulinum toxin is used to block the regeneration of the sectioned muscle to prevent consecutive structural ageing.
More typically, botulinum toxin can also be used to optimize the anti-ageing surgical outcome by treating the areas not operated on (for instance, bitterness fold treatment in the case of concentric malar lift-type surgery) or for improved results (injection within the fine lines above the mouth, a zone not treated surgically with Face Recurve® surgical procedures).
Filling product injections
In the early stage of the aging process, if the patient’s body weight has remained normal when getting older, botulinum toxin injections (used to hamper resting muscle tone and contraction strength) can be successfully associated with moderate filling of the hollow areas caused by fat transfer. Such submuscular filling provides for reshaping and curving the marker fascicles through deep filler injections.


On the other hand, in older subjects, one should absolutely avoid the pitfall consisting in trying to absorb the excess skin at all costs by using a great deal of filler, which may induce puffiness.
Surgical techniques
Localised Face Recurve® surgeries
In structural aging management, Face Recurve® is a new step towards making up for the gap between cosmetic surgery and facelift. Face Recurve® is recommended in structural ageing for the local treatment of the median area (tear trough, naso-labial folds, jowls, bitterness folds, cervical bands) when excess skin has not actually set in as yet: the face is marked but the skin remains tonic. Face Recurve® is also recommended complementarily to previous facelift whenever the results on paramedian ageing have proved insufficient.
The surgeon uses a small incision to cut one or several marker fascicles and puts back to its original place the fat that had been expelled through the action of these fascicles over time. The convexity of the facial expression muscles is thus restored. The patient looks younger through local restoration of the anatomic features best matching those of his/her youth. Very specifically targeted injections of botulinum toxin are carried out during surgery to prevent muscle regeneration of the age marker fascicles. A number of sports injury medicine-related works show that putting a muscle at rest during the healing phase prevents its later recovery.
The procedure is done without the patient being hospitalized. It can be carried out under local anesthesia or assisted local anesthesia depending on the number of zones treated.
Through the action of Face Recurve® on specific marker fascicles it has become possible for the first time to manage simultaneously the consequences (excess skin and sagging) and the primary cause (marker fascicles) of ageing.
Performed singly, the Face Recurve® procedure is therefore not associated with any facelift, since excess skin is not managed thereby. But it is a new type of anti-age surgery which turns out to be quite effective in that it allows both to treat structural aging and to block its further progression.
Cervicofacial Face Recurve® Lift

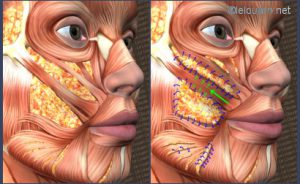
Cervicofacial Face Recurve® lift
Cervicofacial lift
Blue-colored area = detachment area
Blue line = scar
+ Face Recurve®
In yellow = the AMF treated during the procedure
In red = section points of the fascicles
=> action on the upper aspect of the naso-labial fold, the bitterness fold, the jowl, the cervical bands.
In pink = horizontal plication of the lateral platysma muscle to treat the submandibular gland.
The cervicofacial lift is the most frequently used facelift, and it is effective from the neck to the temples. Its intent is to treat skin and muscle sagging and loosening at the facial and neck levels. When cervicofacial lift is conducted using conventional techniques, it is less effective on the median zone of the face than laterally. Hence, its effect is rather limited and often not stable enough as far as structural aging is concerned (i.e., naso-labial folds, bitterness folds and cervical bands). Muscle resection and specific replacement of fat volumes through the Face Recurve® technique must be combined therewith during the procedure, in order to better manage the paramedian folds of the surgical area (the LAN fascicle for the upper aspect of the naso-labial fold, the DAO fascicle for the bitterness fold and the anterior and lateral platysma muscles for the cervical bands). When cervicofacial lift and Face Recurve® are combined to act on the paramedian folds, the procedure is referred to as cervicofacial Face Recurve® Lift.
When using the Face Recurve® Lift, it is no longer necessary to eliminate the after effects of the action the mimic muscles by using lifting skin traction or filling. Any excess skin is removed and the volume masses are restored strictly where they used to be originally, while the paramedian folds are treated locally. In this way, any drawn appearance (given by pulling the skin too tautly to obtain an effect on the median fold which lies at some distance from the scar) or puffiness (due to excess use of fillers to conceal the hollows and to absorb any loose skin) is avoided.
As an example, in the past the jowls used to be treated during the facelift by pulling the skin as far back as possible towards the ear. However, one could not make the skin resist the repeated action of the expression muscle tugging the jowls downwardly (pouting) by merely pulling on it. Henceforth, owing to the appropriate sectioning of the marker fascicle responsible for the jowls (DAO) and the replacement of the fat masses that had been expelled by DAO contraction, the facelift per se strictly involves excess skin resection. In terms of jowl management, results are more effective, natural-looking and stable.
The anatomic features are thus restored in a way to match as closely as possible the young subject’s, while resection provides for blocking the deleterious action of the marker fascicles and, hence, prevents further structural age-caused damage.
From now on, surgery can be counted as part of the global anti-age strategy. The goal of the Face Recurve® Lift is not to change the shape of the face but to secure the most natural looking and durable results that can be obtained, i.e.:
– closest possible restoration of the young subject’s original anatomy: fat transfer (Face Recurve®) and renewed musculocutaneous tonicity (Facelift);
– coherence between the restored facial structures on the one hand, and the improved cutaneous appearance as obtained by skin rearrangement, on the other hand;
– reduced necrosis risks due to restrained skin traction procedures (thanks to the locally-oriented action of Face Recurve®);
– prevention of secondary structural ageing by sectioning of the age marker fascicles (Face Recurve®).
Concentric Malar Lift*

When eyelid surgery is combined with a Face Recurve® procedure limited to the palpebral region, it is referred to as Concentric Malar Lift . This involves a Face Recurve® and a facelift of the central portion of the face. One should stress that the eyelids constitute a zone of very delicate, and hence fragile, but very much active tissues. Therefore, it is not rare to have to treat this area for ageing much sooner than the rest of the face, even before the age of fifty.
The concentric malar lift allows restoring the initial structures of the central area of the face in order to obtain harmonious rejuvenation of this region. The concentric malar lift is effective on the lower eyelids, the hollowing of the eyes, the tear trough, the cheekbones and the naso-labial folds by way of a scar running flush to the eyelashes of the bottom lids. The volumes are lifted concentrically towards the orbit in their original location, and not upwards or outwardly towards the temples which is not where they originate.
The procedure may be conducted :
– either separately on an outpatient basis (neurolept-anesthesia and a few hours’ stay at the clinic)
– or simultaneously without any visible scar with a Face Recurve® surgical treatment of the lower part of the face (involving the bitterness folds, the jowls and the cervical bands)
– or else, associated with a cervicofacial Face Recurve® Lift procedure (with visible scar).
A few secondary consequences of the Face Recurve® concept.
Normally, if one is to adhere to the Face Recurve® concept, one should:
Stop the facial gymnastic sessions used to make the face retrieve its younger look, since these actually promote the ageing process. The facial expression muscles are the only striated muscles (for voluntary movement) in our organism to possess one bone insertion and one skin insertion. All the other striated muscles (body and face) have their extremities fixed to stable structures (bone, ligaments) with a joint in between to allow for movement. This specific feature is significant because the ageing process taking place differs according to the type of insertion. Thus, regarding the body muscles, the longer they are kept active – though reasonably so – the more likely the functional structures are to stay “young” longer. Conversely, as far as facial expression muscles are concerned, the more active they are the earlier the ageing process will set in.
And avoid using hanging sutures (serrated stitches, curl lift, Russian stitches…) which, as a rule, shift the soft structures up and outwardly, i.e. out of their original position, which often causes the features to be changed rather than giving them a younger appearance. For instance, by lifting the cheekbones, those will cause the hollow rings under the eyes to become more visible, so as to make it necessary to fill them in with a filler. Given the risks and disadvantages linked to the use of sutures, it seems advisable to use only the filler when a change of looks is not wanted.
Moreover, hanging sutures tend to freeze the appearance, which is contrary to dynamics of a young face. Finally, the efficacy of such sutures is often low at the beginning of the aging process (because the problem at this stage does not lie with the sagging of excess skin) and insufficient later on (insofar as to be really effective, it becomes necessary to remove the excess skin).
Face Recurve® : a global management strategy for structural aging (at each treatment phase).
As stated earlier, Face Recurve® has not only caused a real turnabout of the way the mechanism of structural aging of the face used to be thought of, but it has lead to profound changes in the anti-age therapeutic strategy for structural aging both surgery- and medicine-wise.
Phase 0
(around 25-30 yrs)
Toxin Recurving®

Botulinum toxin may be used to prevent time-related AMF shortening to decrease muscle tone without reducing maximum contraction strength.
Phase 1 (normally around 30-35 yrs)
Toxine Filler Recurving®

Botulinum toxin is still used to obtain an effect on muscle resting tone, but it is also used in other locations to hamper contraction strength in order to obtain an effect on facial expression lines, as in the case of crow’s feet. Additionally, it is associated with filling of the areas that have been hollowed because of fat expulsion using deep filler injections to recurve the age marker fascicles.
Phase 2
(usually around 40-45 yrs) :
Face Recurve®

Face Recurve® is recommended to treat structural ageing involving the median zone (naso-labial folds, jowls, bitterness folds, cervical bands), whenever excess skin has not yet become a problem: the features are marked but the skin is still firm. Or else, supplementary to previous facelift surgery, wherein the outcome proved inadequate in terms of paramedian management.
Using a short incision, the surgeon sections precisely, one or several age marker fascicle(s), and puts back in its original place the fat tissue that had been expelled through the action of the AMFs over time. In this way, the convexity of the mimic muscles is restored. The patient looks younger and his/her anatomic features are closest to those he/she once had.
Face Recurve® is not quite the same as a facelift since the skin is not drawn, but it is a new anti-age surgical technique of significance, since it provides simultaneously for treating the structural ageing-related sequelae and for curtailing the secondary structural ageing process.
Phase 3
(most often after age 50) :
Face Recurve® Lift

Whenever structural aging has set in, excess skin becomes apparent and the phenomenon is made worse secondarily by the gravity factor. AMFs section procedures together with specific fat volume replacement as provided by the Face Recurve® procedure must then be combined with excess skin removal, i.e., the facelift surgery.
References
1 – LE LOUARN C. : Emploi de l’acide hyaluronique selon le concept du Face Recurve® : vacuum technique et interpores technique
Use the hyaluronic acid according to the concept Face Recurve®: vacuum technical and interpores technical
Ann Chir Plast Esthet. 2007 Oct 17;
http://dx.doi.org/10.1016/j.anplas.2007.05.016
http://www.ncbi.nlm.nih.gov/pubmed/17942211
2 – LE LOUARN C : Toxine botulique et Face Recurve® : action sur le tonus de repos et la régénération musculaire
Botulinum toxin and the Face Recurve® concept: decreasing resting tone and muscular regeneration
Ann Chir Plast Esthet. 2007 Jun ; 52(3):165-76.
http://dx.doi.org/10.1016/j.anplas.2006.11.007
http://www.ncbi.nlm.nih.gov/pubmed/17320262
3 – LE LOUARN C, BUTHIAU D, BUIS J. : Structural aging: the Facial Recurve concept
Aesthetic Plast Surg. 2007 May-Jun ; 31(3):213-8
http://www.ncbi.nlm.nih.gov/pubmed/17380358
4 – LE LOUARN C, BUTHIAU D, BUIS J. : The Face Recurve concept: medical and surgical applications
Aesthetic Plast Surg. 2007 May-Jun;31(3):219-31; discussion 232.
http://www.ncbi.nlm.nih.gov/pubmed/17484058
5 – LITTLE J.W. : Structural aging: the facial recurve concept
Aesthetic Plast Surg. 2007 Nov-Dec ; 31(6):754-6.
http://www.ncbi.nlm.nih.gov/pubmed/17985177
6 – LE LOUARN C, BUTHIAU D, BUIS J. : Rajeunissement facial et lifting malaire concentrique : le concept du FACE RECURVE®
Facial rejuvenation and concentric malar lift: the FACE RECURVE concept
Ann Chir Plast Esthet. 2006 Apr ; 51(2):99-121.
http://dx.doi.org/10.1016/j.anplas.2005.12.016
http://www.ncbi.nlm.nih.gov/pubmed/16530316
7 – LE LOUARN C, BUTHIAU D, BUIS J. : Treatment of depressor anguli oris weakening with the face recurve concept
Aesthetic Surgery Journal, Volume 26, Issue 5, Pages 603-611C.
http://dx.doi.org/10.1016/j.asj.2006.08.001